“A third of this country thinks health care is a basic human right and the government should finance the whole shebang; another third thinks health care is a market good that should be earned, with the government banished from sight; a middle third does not know what it thinks, only what it fears, based on the latest anecdote about Medicare fraud, insurance company abuse, government incompetence, or medical private profiteering in their local news cycle. If nothing else, ObamaCare has proven to be a dark mirror on our most deeply embedded cultural conflicts, from the death panel freakshows to the neanderthal discussion on birth control.”
- JD Kleinke
"It’s always a bit strange to hear people with government-funded single-payer health plans describe the need for other Americans to be free from health insurance. But after the aggressive battery of questions from the court’s conservatives this morning, it’s clear that we can only be truly free when the young are released from the obligation to subsidize the old and the ailing."
- Dahlia LithwickWEDNESDAY UPDATE
Three days of argument, six hours total, 427 pages of transcript spanning four areas of contention: AIA "Ripeness," Individual Mandate, Severability, and Medicaid "coercive" expansion.
Lotta stuff goes down with the ship should they strike PPACA in toto. e.g., just the section pertaining to much of my work going forward.

In addition to much more. Dunno; maybe a lot of this stuff is indeed a waste (as critics have said of ARRA/HITECH as well). But, do we seriously believe that competing for-profit entities will rush to fill the breach to do a transformative collective altruistic Kumbaya for the benefit of the commonwealth?
Indeed. e.g., from HealthCare.Gov:

The Health Care Blog posted a nice compendium of the dueling rhetorical analogies at Orals.
One way or another, we'll know in about three months. So, what to do while we wait? How about Joe Flower's comment in “Three Strategies for the Health Care Industry While Reform’s in Limbo”:
"At the end of the day, it is a very hard thing to ask the federal court to strike down any act of Congress, particularly one like this that has the eyes of so many Americans on it. One thing here is that a lot of the concerns are policy concerns against the act and not constitutional concerns. In circumstances like this, in which there is no clear constitutional law that blocks the government from doing what it is doing, it is going to be very difficult to strike it down."
- Neal Katyal, Georgetown law professor and former acting solicitor general, May 2010-June 2011REWIND: "One thing here is that a lot of the concerns are policy concerns against the act and not constitutional concerns"
Indeed. e.g., from HealthCare.Gov:
Title III. Improving the Quality and Efficiency of Health Care
The Act will protect and preserve Medicare as a commitment to America’s seniors. It will save thousands of dollars in drug costs for Medicare beneficiaries by closing the coverage gap called the “donut hole.” Doctors, nurses and hospitals will be incentivized to improve care and reduce unnecessary errors that harm patients. And beneficiaries in rural America will benefit as the Act enhances access to health care services in underserved areas.
The Act takes important steps to make sure that we can keep the commitment of Medicare for the next generation of seniors by ending massive overpayments to insurance companies that cost American taxpayers tens of billions of dollars per year. As the numbers of Americans without insurance falls, the Act saves taxpayer dollars by keeping people healthier before they join the program and reducing Medicare’s need to pay hospitals to care for the uninsured. And to make sure that the quality of care for seniors drives all of our decisions, a group of doctors and health care experts, not Members of Congress, will be tasked with coming up with their best ideas to improve quality and reduce costs for Medicare beneficiaries.
The Secretary has the authority to take steps to strengthen the Medicare program and implement reforms to improve the quality and efficiency of health care.
Title IV. Prevention of Chronic Disease and Improving Public Health
The Act will promote prevention, wellness, and the public health and provides an unprecedented funding commitment to these areas. It directs the creation of a national prevention and health promotion strategy that incorporates the most effective and achievable methods to improve the health status of Americans and reduce the incidence of preventable illness and disability in the United States.
The Act empowers families by giving them tools to find the best science-based nutrition information, and it makes prevention and screenings a priority by waiving co-payments for America’s seniors on Medicare.
The Secretary has the authority to coordinate with other Departments, develop and implement a prevention and health promotion strategy, and work to ensure more Americans have access to critical preventive health services.
Title V. Health Care Workforce
The Act funds scholarships and loan repayment programs to increase the number of primary care physicians, nurses, physician assistants, mental health providers, and dentists in the areas of the country that need them most. With a comprehensive approach focusing on retention and enhanced educational opportunities, the Act combats the critical nursing shortage. And through new incentives and recruitment, the Act increases the supply of public health professionals so that the United States is prepared for health emergencies.
The Act provides state and local governments flexibility and resources to develop health workforce recruitment strategies. And it helps to expand critical and timely access to care by funding the expansion, construction, and operation of community health centers throughout the United States.
The Secretary has the authority to take action to strengthen many existing programs that help support the primary care workforce.
Title VI. Transparency and Program Integrity
The Act helps patients take more control of their health care decisions by providing more information to help them make decisions that work for them. And it strengthens the doctor-patient relationship by providing doctors access to cutting edge medical research to help them and their patients make the decisions that work best for them.
It brings greater transparency to nursing homes to help families find the right place for their loved ones and enhances training for nursing home staff so that the quality of care continuously improves. The Act promotes nursing home safety by encouraging self corrections of errors, requiring background checks for employees who provide direct care and by encouraging innovative programs that prevent and eliminate elder abuse.
Finally, the Act reins in waste, fraud and abuse by imposing tough new disclosure requirements to identify high-risk providers who have defrauded the American taxpayer. It gives states new authority to prevent providers who have been penalized in one state from setting up in another. And it gives states flexibility to propose and test tort reforms that address several criteria, including reducing health care errors, enhancing patient safety, encouraging efficient resolution of disputes, and improving access to liability insurance.
The Secretary has new and improved authority to promote transparency and ensure that every dollar in the Act and in existing programs is spent wisely and well.
Title VII. Improving Access to Innovative Medical Therapies
The Act promotes innovation and saves consumers money. It extends drug discounts to hospitals and communities that serve low-income patients. And it creates a pathway for the creation of generic versions of biological drugs so that doctors and patients have access to effective and lower cost alternatives.
The Secretary of Health and Human Services has the authority to implement these provisions to help make medications more affordable.
Title X. Reauthorization of the Indian Health Care Improvement Act
The Act reauthorizes the Indian Health Care Improvement Act (ICHIA) which provides health care services to American Indians and Alaskan Natives. It will modernize the Indian health care system and improve health care for 1.9 million American Indians and Alaska Natives.
The Secretary, in consultation with the Indian Health Service, has the authority to implement the Indian Health Care Improvement Act.Now, maybe one can legitimately be dubious with respect to the wisdom/prospective utility of one or more of these ostensibly noble provisions. It escapes me, however, how they could be found to be "unconstitutional," -- beyond the scope of legitimate Congressional authority.
If the decisions of individuals not to eat broccoli and not to buy burial insurance had similar effects on interstate commerce, then it might also be appropriate for the national government to intervene. But the hypotheticals are, quite frankly, ridiculous. They are bad arguments to which any first-year law student knows the answer. If the conservative justices, who are, after all, very good lawyers, rely on such arguments to defend a decision to invalidate the Affordable Care Act, then we know something else is going on.
How justices who purport to celebrate their commitment to judicial restraint and judicial modesty could even imagine striking down this law on such transparently weak grounds is beyond comprehension. For that reason, I don’t believe they will do so. If they do, it will be (another) dark day for the Supreme Court, which already labors under a cloud of public disillusionment after its decisions in Bush v. Gore and Citizens United.
- Geoffrey R. Stone, Esq, Edward H. Levi Distinguished Service Professor of Law, University of Chicago.

The Health Care Blog posted a nice compendium of the dueling rhetorical analogies at Orals.
- Is mandating health insurance like mandating that people buy cell phones to call 911? (Chief Justice Roberts).
- Is the mandate like a requirement that we buy insurance to pay for our own burial services? (A macabre Justice Alito, who’s right: we’re all going to die).
- Is the mandate like forcing us to buy broccoli? (Justice Scalia, invoking the dreaded broccoli analogy, which is apparently one of the parade of horribles that logically flows from the health insurance mandate, a canard that David Orentlicher has exposed).
- Is it like forcing us to buy cars? (Chief Justice Roberts and later, Justice Scalia, referring to the government’s reply brief, which tried to distinguish a federal mandate that we buy U.S. automobiles from the insurance mandate).
- Is it like imposing a duty to rescue strangers in trouble, like a “blind man walking in front of a car”? (Justice Kennedy).
- Is it like setting phone rates to require that some callers subsidize others? (Solicitor General Don Verrilli).
- Is it like requiring everyone to join an exercise club? (Justice Scalia).
- Is it like mandatory inoculation during a pandemic? (Justice Breyer, perhaps inspired by the movie Contagion).
- Is it like forcing people to deposit all their money in the Bank of the United States? (Justice Breyer’s colloquy with Paul Clement, counsel for the state plaintiffs, invoking McCulloch v. Maryland).
- Would it be like the federal government requiring us to buy car insurance if states didn’t already do so? (Justice Sotomayor, to whom Paul Clement responds that there are lots of people in Manhattan that don’t drive cars. True, but we all have bodies, which require regular tune-ups and sometimes major repairs).
- Would it be like Congress forcing everyone to buy “a great new wonder drug”? (Paul Clement).
- Is it like growing wheat (Wickard v. Fillburn), or weed (Raich), or carrying guns near schools (Lopez), or committing violence against women (Morrison)? Note that these are the four most direct Commerce Clause precedents, which get comparatively buried during oral argument, amid all the analogy-searching.
- Is it like Congress requiring everyone to buy an electric car? (Paul Clement, who is hitting his stride by this point).
- Is it like requiring us to buy anti-pollution devices or low-emission mufflers for our cars? (Justice Breyer, who is not).
- Is it like requiring that everyone buy private mortgage insurance? (Michael Carvin, counsel for the private plaintiffs).
- Is it like requiring some pesticides rather than others in food? (Justice Sotomayor).
- Is the decision not to purchase health insurance like local manufacturing, which is regulated federally because some products might, eventually enter interstate commerce? (Justice Sotomayor).
I also enjoyed the arduous nit-picking over the framing semantics of key words and phrases.
"In the animal kingdom, the rule is, eat or be eaten; in the human kingdom, define or be defined."
- Thomas Szasz, MD
__
"There's an Alice-In-Wonderland aspect to this debate since the politics of the individual mandate intimately intersect with the political careers of this year's presidential nominees. One candidate even pretends his pioneering role is somehow irrelevant because of the 10th Amendment or some other rhetorical sleight of hand.
Supreme Court justices are political animals and they're more than willing to take precedents and cast them overboard if it furthers their own activist desires (e.g., Citizens United). If this case were decided purely on the basis of stare decisis, there would be no question about the legality of the mandate. But it's being decided in a political arena, one where the actors wear black robes and over their campaign buttons.
The ideological question that is the central to our government is whether the Constitution should reflect the country of the 21st century or the 18th century. Thomas and Scalia are more than willing to turn back the clock to an agrarian republic where simplicity ruled the lives of citizens. Today, it's complexity that rules, mostly because of industrialization and economic stratification, and as a result of that, a citizenry ruled by economic forces the Founding Fathers couldn't foresee. A Constitution that doesn't reflect the physical reality of this republic is a straitjacket. And a jurisprudence that indulges nostalgic daydreams of yeoman farmers and town halls is probably closer to nihilism than virtue."
- Walter HallIf that doesn't suffice, consider "ObamaCare Is On Trial. So Is the Supreme Court" by Jonathan Cohn:
...Virtually everybody agrees that a vote to strike down the Affordable Care Act would be five to four—a bare majority. And it would be a bare partisan majority, with the five Republican appointees overruling the four Democratic appointees. The decision would appear nakedly partisan and utterly devoid of principle. Appearances would not be deceiving.
The second distinction is even more more significant. Today Brown is a nearly universal icon of social progress, while Roe remains an object of great controversy. But, for better or for worse, both cases represented efforts to change the everyday reality of American life. With Brown, the justices were tearing down barriers to racial equality; with Roe, the justices were eliminating laws that prevented access to abortion.
But in this case, nobody has said they want to stop government from providing universal access to health care. On the contrary, the plaintiffs have stated that a program like Medicare, in which the government provides citizens with insurance directly, would be clearly constitutional. They’ve also stated that a scheme of compulsory private insurance would be constitutional if somehow the government could make people buy it when they show up at the hospital—suggesting, as Elena Kagan stated, that the only problem with the Affordable Care Act is temporal.
Most amazing of all: The plaintiffs have conceded that a universal health insurance program would be constitutional if, instead of penalizing people who decline to get insurance, the government enacted a tax and refunded the money to people who had insurance. As Sonia Sotomayor noted, functionally such a scheme would be exactly the same as the Affordable Care Act. Both the plaintiffs and some of the skeptical justices have also indicated that the Affordable Care Act would be constitutional if the law's architects had simply used the word "tax" to describe the penalty.
Think about that for a second: If the justices strike down the Affordable Care Act, they would be stopping the federal government from pursuing a perfectly constitutional goal via a perfectly constitutional scheme just because Congress and the Preisdent didn’t use perfectly constitutional language to describe it. Maybe labels matter, although case law suggests otherwise. But do they matter enough for the Court to throw out a law that will provide insurance to 30 million people, shore up insurance for many more, and help to manage one-sixth of the American economy? It wouldn’t seem so.
Of course, the conservative justices who would invalidate the Affordable Care Act may not hold the law in especially high regard. Samuel Alito, in particular, suggested during oral argument that he had serious problems with younger, healthier people subsidizing, via their insurance premiums, the medical expenses of older, sicker people—which just happens to be the defining feature of Medicare, Social Security, and every other social insurance scheme on the planet.
Alito is entitled to his opinion about what makes for good legislation. But he’s not entitled to impose that opinion on the country and his colleagues aren’t, either. Their job is to determine whether a law is constitutional, not whether a law is wise. And the more significant the law, the more unambiguous their judgment ought to be.Indeed, indeed.
One way or another, we'll know in about three months. So, what to do while we wait? How about Joe Flower's comment in “Three Strategies for the Health Care Industry While Reform’s in Limbo”:
The whole debate over the PPACA has obscured the fact that there is a massive shift in the economic structure of healthcare that we are seeing the beginnings of, and that will accelerate over the next few years, and that will likely change the way we do business in this field massively, leading, I believe, to much cheaper healthcare done much better for many more people. Those parts of the PPACA you refer to are small catalysts of some of this change, but are not the change itself.
ACOs themselves, in most of the forms we are seeing, are not actually business models. In ACOs the government is saying, in effect, “find ways to cut your own revenue stream, follow a lot of restrictions and procedures perfectly, and we will let you keep some portion of the money you saved us.” That’s not a sustaining economic model. Other models, like the Alternative Quality Contracts of the Massachusetts Blues, actually are a business model — organizations under them make money by saving the system money. This is a crucial difference. If you can base your business on making money by saving the system greater amounts, you have a sustainable business model that drives the system toward leaner, more effective territory very quickly.
So I would say to healthcare execs: Don’t pay too much attention to what happens to reform. Plan your strategy right now to leapfrog beyond it to completely new business models, before your rivals do, and before new organizations are formed to take the opportunity away from you.___
BACK TO "MY SCOPE"

Just downloaded this to my Kindle. Looks very interesting. to wit, at random:
A good read thus far. Good coverage of the topics.0: Health IT Humility
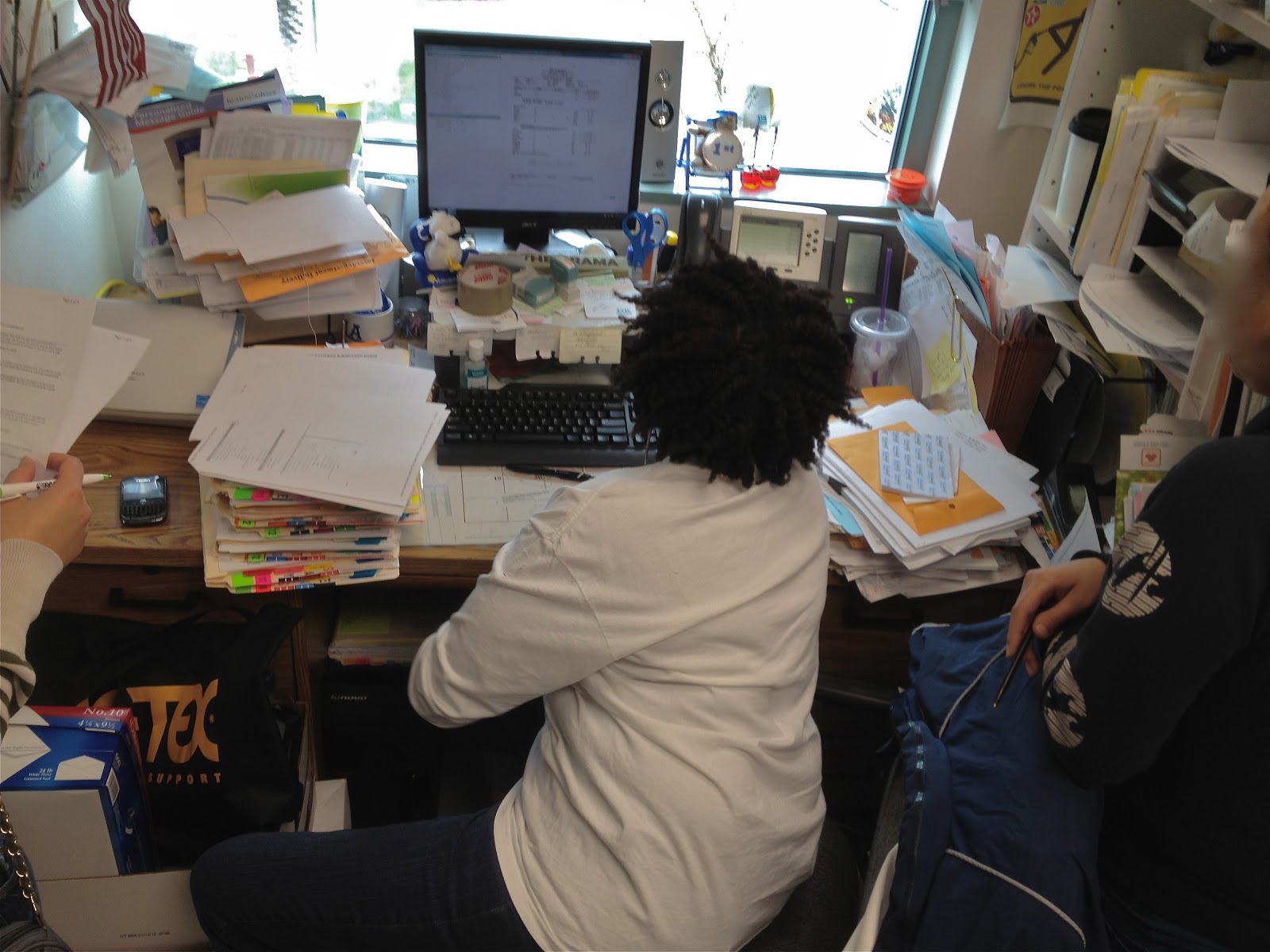
The first thing that computer technologists must free themselves from is the notion that computers are the “solution” to information flow in a clinical environment. If computer specialists do not understand everything that a paper process is doing, or fail to respect the ways in which a paper-based information system handles something well, then they will appear arrogant to the clinical staff, who understand perfectly how effective the paper forms can be. When you introduce a computer system that makes a process that used to take 30 seconds take 10 minutes, then your solution will instantly be met with derision by clinical staff who are already overworked.
If you want a concrete example of how good paper is, consider the surgical checklist movement that has been growing in popularity. Studies have shown that this simple information intervention, which uses either a paper form or a whiteboard, has improved patient safety on the operating table more than any surgical technique advancement in the equivalent time frame. The next time you are feeling smug about your awesome health IT plans, keep in mind that this simple information intervention, which required no software at all, might be the most effective information-based intervention of the decade.
Trotter, Fred; Uhlman, David (2011-10-07). Meaningful Use and Beyond: A Guide for IT Staff in Health Care (Kindle Locations 1544-1554). OReilly Media - A. Kindle Edition.
Chapter 10
Ontologies:
Practically speaking, an ontology is just a fancy word for a dictionary. More specifically, an ontology is a way of structuring knowledge, by coding complex concepts into simpler terms. Beyond that, ontologies vary widely in the level of complexity given to structuring the relationships between the terms. Some people use the term ontology in healthcare to refer to only systems that are capable of deeply modeling clinical information. Others use the term to refer generally to all types of abstract health care data sets. Sometimes, people speak about ontologies in terms of codes, code sets, or coding processes. This chapter will cover both important sources of clinical coding systems or ontologies, of several types.
The basic problem that clinical ontologies seek to address is the difficulty that automated processes have with synonyms. Heart attack, cardiac arrest, and myocardial infarction, as well as the acronyms MI or AMI, can all be used to describe the same event. Having multiple terms for the same thing is difficult if you want to fully automate any clinical information process. An ontology solves this problem by noting that the terms heart attack, myocardial infarction, MI, and AMI really are the same thing, and cardiac arrest, like cardiac arrhythmia are related terms, but not synonyms for those concepts.
Traditionally the academic study of ontologies has been of interest to philosophers, computer scientists, and cognitive scientists, who are deeply concerned with the mechanisms by which humans encode knowledge. We will mostly be ignoring the high-brow, but interesting, philosophical issues with ontology unless they specifically impact some aspect of the practical use of ontologies in healthcare. If you are already familiar with the concepts of ontologies you might be somewhat offended by the way typical medical ontologies ignore simple obvious principles that the science of ontology provides. Most medical ontologies are either irredeemably poor as knowledge representation schemes, or so consistently abused in practice that they might as well be. Moreover, no chapter on medical ontologies could begin without the admission that the coverage of ontologies is complex enough to merit a book on its own, and that the licensing of medical ontologies is so convoluted and inconsistent that this chapter certainly should not be taken as anything close to legal advice.
(Kindle Locations 3784-3804).Chapter 4: The Bandwidth of Paper
...Consider the blank sheet of plain white paper. A sheet of paper can become legal notes for a lawyer, the design of a machine or circuit for an engineer, the careful drawing of a building for an architect, and notes about a patient for a doctor. When you account for paper airplanes and origami, paper has a wonderfully large number of wonderful uses.
The powerful aspect of a paper chart is that there is never a limitation of the type or content of data that can be added. If it can be written or drawn, it can be added as needed.
The recently released Apple Retina display is 326 pixels per inch (PPI), and normal humans cannot see clearly past 300 PPI. In the HDMI video standard, monitors must support 30-bit color on the low end. An 8-1/ 2 x 11-inch sheet of paper comes out to 8,415,000 pixels at 300 DPI (more HD than the most uber-HD monitors now available).
Assuming they support a 30-bit color depth, this means that they are supporting 252,450,000 bits per image, or about 31 MB per image. Of course, the human eye is capable of seeing many of these pages per second, but the real of the paper system is a human’s ability to change sheets of paper quickly. Assuming the doctor was really moving, he might see 5 pages per second. That puts the bandwidth of paper at something like 1262.25 megabits per second (Mbps). In comparison, a good broadband Internet connection runs at about 5 Mbps, which is enough to stream movies. If you account for the fact that a doctor might be dynamically ignoring 995 pages of medical record to look at the right 5 pages, and then considered her rate of consumption at 1,000 pages per second, the bandwidth of paper is faster, by far, than any computer network in practical existence. All of these numbers are estimates, but it would be difficult for anyone not to concede that the actual bandwidth of paper-to-brain is pretty fast.
Moreover, it is easy to make paper better at any given information task. It is simple for any doctor to use a computer or photocopier to print lines and labels all over the blank sheet of paper, turning a simple sheet of paper into a form. Paper forms in healthcare are far more potent than in most industries.
When doctors look at a paper form, they feel no loyalty to the lines and check boxes. Doctors are not mere paper pushers or automatons who fill in everything in triplicate. Doctors feel comfortable drawing “outside the lines” and because they often create their own forms, and are frequently the only readers of their own completed forms, the paper-based patient data system melds easily with the mind of the designing physician. This is all just the benefits of a single paper form; when you add a folder to keep groups of forms together, it becomes even more powerful.
Instructions, diagrams, complaints, compliments, questions, answers, tables, pictures, reports, receipts, faxes, and, of course, post-it notes can all be added to a paper chart, normally just a folder, with ease. Doctors’ handwriting is famously illegible, but they rarely need to actually read the entire contents of a chart. They need to be able to use the written record of what they wrote to jog their memory: what is special or different about this patient, what are the next steps in the treatment? During typical operations the chart need only indicate what the next step is to the doctor who made it. But it is still powerful enough to hold the entire history (assuming the handwriting problem is addressed), for the rare occasions when it is important to look at everything.
The nurse who filled out the example form in Figure 4-1 also wrote “Lung DZ” in the history section. That phrase means “Lung Disease,” and is a wonderful example of medical abbreviations, an important part of the paper chart that will make the jump to electronic charts. Medical abbreviations are now largely standardized, after a substantial number of medical errors occurred because of nonstandard abbreviations. The standardization of abbreviations bounds written data, even on paper forms. Once medical abbreviations became standardized, they provided a clear enough shorthand for common medical terms that they could safely be recommended for use. But this is only possible when the mapping between abbreviations and longer terms is perfectly understood and mostly identical everywhere. That mapping, between abbreviations and longer terms, is in fact a healthcare ontology, one that performs well on paper. We will discuss medical abbreviations further in Chapter 10.
Workflow Tokens
Individual paper forms are typically tokens in a complex clinical workflow. The nurse fills out a form when the patient arrives and gives the patient a copy. The patient then takes it to the X-ray department. The X-ray department performs an X-ray and gives the results (on paper and film) to the patient to take upstairs to a particular doctor. The nurse in the waiting room takes the papers and film, and deposits them in a wall-mounted box outside an exam room, and escorts the patient into the room. Each of the steps can have a check box on the form itself, so that the patient knows just where to go next, and if she gets lost (and who doesn’t in a hospital?) anyone can look at the form and show the patient where to go next. There are thousands of variations on this basic theme to accommodate the various needs of different clinical organizations.
This is an important insight that merits highlighting: even the paper chart (i.e., the bundle, not just a single form) is not just a paper record of a patient’s healthcare history and current status. It is also a token in a clinical workflow. Considering the record without considering the workflow is a simple mistake that is easy for technologists to repeatedly make. To prevent this mental error, try to adjust your mental imagery of a paper chart into something dynamic and moveable in nature. One of the authors tries to imagine the record as a manila folder with little wheels attached to it. That is a pretty silly mnemonic, but it works.
Some clinics use colored folders to enable different workflows. They place the chart in a green folder and send the patient to the green waiting room. A red folder might mean that a patient is waiting in the red waiting room, and in another clinic it might mean that a patient needs to have blood drawn. As we say elsewhere, there is no such thing as a typical healthcare workflow. At a minimum the paper chart is the home base to the various paper forms that enable different clinical workflows, and the whole contents must be copied to other organizations or departments when the patient moves. So the paper chart is always a workflow token, exercised to different degrees, in different organizations.
Often, a paper form will have been designed and cemented in the workflow so long ago that no current employee can remember why the form was designed in a particular way. Be very careful of this, because as you seek to replace the form in the workflow with software, you might discover that what you considered an incidental aspect of the form’s design was actually solving some important important problem in another portion of the workflow that you did not fully understand.
Why Leave Paper?
Paper is an excellent record of clinical care, to the degree that the data does [sic] not need to move. It is a perfect healthcare record to the degree that healthcare is provided by a single clinician, looking at a patient chart and the patient all at the same time. Modern healthcare is no longer a one-doctor, one-record, one-patient game. The coordination of care for a patient requires that critical information be moved from where it is to where it needs to be, on time. Sometimes the paper chart moves fast enough. Most of the time it does not. God forbid a paper chart should be lost.
The first thing that people assume when you say “coordination of care” is that you mean between-organization coordination. But the primary benefit of EHR systems is that they coordinate care within a healthcare organization. This is why EHR adoption has been so strongly correlated with the size of a clinical organization. The more an organization needs to communicate with itself about a given patient, the greater the benefit of an EHR system. Conversely, single-clinician practices get the least benefit from computerization.
There are classes of medical errors that are clearly related to the information not moving fast enough, like a patient’s allergies or current medication list not being with the nurse when a new drug is given to a patient. Many preventable medical errors go away entirely when you measure them, which means they mostly disappear whenever manual observation occurs. The spread of infections due to clinicians forgetting to wash their hands is a good example of this. The only real solution is to measure these types of behaviors all the time electronically, preferably preventing rather than merely chronicling the errors in question. Real-time workflow interruption can only occur when data values can spawn real-world stimuli (like flashing lights or beeps), and that means software.
Lastly, paper charts are difficult to study en masse. Doctors can easily look at a single paper chart and see how a patient with diabetes is doing, but they cannot get same information about all of their patients with diabetes without doing costly and slow chart reviews. Paper chart reviews simply cannot serve to inform a profession that changes as fast as healthcare does.
Paper data is [sic] trapped, inactive, and difficult to study. If paper could shout, there would be no need for EHR systems. (Kindle Locations 1446 -1542)

More to come...